As the unvaccinated cause a Fourth Wave, is it time for mandates?


What if I showed you the evidence that we are about to go into a horrendous Fourth Wave of the pandemic, and a significant change in policy could save lives? What if I showed you that, in six months, the unvaccinated will cost our state at least $15.3 billion, and our country $1.5 trillion dollars, but a $70 jab of a vaccine that is free for the unvaccinated isn’t the only, or even the most expedient, solution? Would you consider that it might be time for some alternatives to vaccination mandates?
This op-ed is for those who decide which policies we implement as we move into the Fourth Wave of COVID-19 deaths. The op-ed isn’t focused on who to blame for the Fourth Wave. It is to focus on what political leaders, particularly on the right, need to do next to soften the blow. So you know where I am coming from, I’ve been intensely researching COVID-19 since January 2020, and writing highly accurate forecasts of where the virus is heading. Since this op-ed is about policy, I need to disclose my politics. I had been a lifelong Republican, until relatively recently. I’m registered nonpartisan. I’m a business owner used to making data-driven financial decisions. I lean toward the libretarian side on both economic and social issues. I’m a fan of The Economist, with its support of free markets and market based solutions. In sum, I would not have guessed I’d be writing an op-ed leaning in favor of mandates. But I’m leaning that way only because we need reasonable alternatives to vaccinating the unvaccinated.
There is no question vaccinations offer the best protection. I know this with certainty because of the study I conducted with Brown University, Harvard, Nevada State Public Health Lab, and Washoe County Health District.
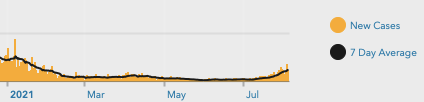
We studied every case in Washoe County from February 1st through July 29th. We analyzed whether the person was vaccinated or not, and the clinical outcomes (hospitalization, death, recovery). During most of this period, cases trended downward, and nearly every case was among someone not fully vaccinated. In mid-May, with cases at historic lows and trending downward, the CDC issued new guidelines that those FULLY vaccinated could remove their masks. Those not fully vaccinated should continue to wear them.
I appreciate the spirit of the CDC guideline, but I didn't think some (many?) of those unvaccinated would keep wearing a mask. Removing a mask for some could create a stigma for others.
Perhaps you noticed the same thing I noticed when I walked into a store: If those unvaccinated were following the guidelines, then when we walked into a store we would have seen about half of adults still wearing a mask.
What did you see? I saw that virtually no one was wearing a mask.
The CDC may have hoped removing the mask for those fully vaccinated would be a good incentive for people to get vaccinated - and a small percentage of people did. But, mostly, the unvaccinated shed their masks -- and many of them shedded virus too, seeding the Delta variant we are experiencing today.
The consequence? Our research into the 6,128 cases the Washoe Health District traced is that 95 percent (5,790) of all cases were among unvaccinated people. Considering that 49 percent of the total population in Washoe was not fully vaccinated as of July 29th, it means that roughly 1 in every 38 unvaccinated people had a confirmed case of COVID. Since not all infections are detected and confirmed, the total infections are likely three times worse… closer to 1 in 13 of unvaccinated people contracted and may have spread the SARS-CoV-2 virus during this six month period.
Hospitalizations follow the same pattern. Out of the 428 hospitalizations, 96 percent (411) were among those not vaccinated. Worse, for those not vaccinated, the median age of hospitalization is 49.2 years old, compared to 71.8 for those very few vaccinated people who were hospitalized.
Let that sink in: 49.2 is the average age of a hospitalized unvaccinated COVID patient.
Compare that to those fully vaccinated. Only 1 in 711 fully vaccinated people had a confirmed case of COVID during this study period. If we apply the same 3x ratio of confirmed cases to likely infections, only 1 in 237 fully vaccinated people got COVID. At such a low rate, the virus would have burned itself out if everyone was vaccinated. We wouldn’t be starting a Fourth deadly Wave if those unvaccinated became vaccinated, or at least wore a mask. Our hospitals wouldn’t be filling up.
The average cost of a COVID hospital stay is $73,000 versus a $70 jab of the vaccine. In less than six months, those unvaccinated racked up over $30 million in hospital bills in Washoe County alone. Worse, 80 unvaccinated people died in this period of time in Washoe County.
The value of a life can’t adequately be represented in dollars. Still, the EPA, FAA, employers and insurance providers do apply what is called a statistical value of a life. The average figure used by the U.S. government to calculate a statistical value of a life is $8.7 million. Multiplying the 80 deaths (all unvaccinated), we arrive at a bill of $696 million - for a total cost to society of $726 million (hospitalizations + deaths), in less than six months.
If you think the statistical value of a life is too high, consider the combined cost in 2021 of the CARES Act plus the reduction in GDP versus the consensus estimate prior to the pandemic. It works out to be $9.2 million per person that died last year. Since then, the average age of those dying of COVID has dropped by more than a decade. COVID is now hospitalizing people in their economic peak. More than 47,000 children under 18 have lost one or more of their parents to COVID-19. $8.7 million per death is likely a conservative estimate of the total economic cost.
To vaccinate every remaining unvaccinated person in Washoe would cost $16.2 million, and could have saved intangible heartache and pain for all the families that experienced senseless COVID hospitalizations and deaths. We could vaccinate all remaining adults in the US for about $9.6 billion.
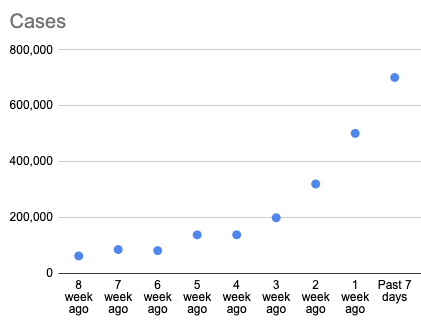
The next six months will be even more expensive. My forecast over the next six months (published in Research World), is for 168,000 incremental deaths in the US, almost entirely among unvaccinated. Hospitalizations will be roughly 5.3 times higher than the death toll at 890,000. The unvaccinated will be dying at a rate higher than any other leading cause of death. Given the surge in cases, and the consistent pattern that roughly 1.5 percent of cases die of COVID-19 a few weeks later, we are headed to around 30,000 deaths over the next month, and likely higher in future months because we have not yet seen the peak of new cases yet.
Alternatives
A vaccine mandate is a logical solution, but the resistance to vaccination isn’t logical. It is deeply emotional for many and fed by misinformation. Are there complimentary approaches to vaccination that offer those not ready, willing or able to vaccinate an alternative? Most conservatives favor market solutions. A market solution pairs individual choice with individual responsibility. Here are a few idea starters for our leaders:
Option 1:
“You choose not to be vaccinated, you get an antibody test and do COVID testing weekly.”
- Part 1: Antibody tests help estimate the level of protection. Private party antibody testing costs $75. Medicare pays about $50. This is relatively inexpensive for someone choosing not to be vaccinated.
- About half the unvaccinated were likely infected at some point, based on my modeling analysis. Some may have had their immunity wane. While vaccines produce about 10x more antibodies than natural recovery, and is the best approach for most people. If the antibodies are sufficient, and someone doesn’t want to get vaccinated, then evidence of antibody immunity means less risk to the person and to the community around the person than someone without sufficient evidence of protective antibodies. This test should be repeated monthly.
- Part 2: Weekly COVID tests for those without sufficient antibody protection, or, testing prior to unmasked activities such as eating at a restaurant (as is common in countries in Europe).
- No cost to unvaccinated. Costs are borne by the taxpayer.
- Optionally, penalties could be assessed for not being tested weekly.
- Benefit to unvaccinated: If you are infected, this allows for early life saving treatments such as monoclonal antibodies, adequate quarantine and, contact tracing.
- Benefit to society: An unvaccinated person that is infected is likely to be detected earlier, reducing the spread. In addition, the interaction with medical staff for the testing may prompt a decision to get vaccinated, thus further reducing risk and cost to society.
Option 2:
“You choose not to be vaccinated, you assume the cost for testing (approximately $50 per week).”
- Exemptions for select reasons, such as the immunocompromised, who can’t be vaccinated.
- Similar to points above, except rather than society paying for the testing, the unvaccinated bears the cost of testing, and penalties for not testing.
- At any point a person is vaccinated, testing expenses are reimbursed.
Option 3:
“You choose not to be vaccinated, you assume the cost for tests and potential hospitalization.”
- Exemptions for select reasons, such as the immunocompromised, who can’t be vaccinated.
- A full market solution is to pair individual choice with the full cost of that choice. You choose not to be vaccinated, you pay for testing and you pay your medical cost (average price tag is $70,000) should you need treatment.
- Similar to a liability waiver, you are acknowledging the inherent risk in being unvaccinated, and that insurance will therefore not cover the risk. The average cost of $73,000 and legally assume all obligations that go with that risk. An alternative is to create a “risk premium” and add a supplemental insurance charge to those who could be vaccinated, but choose not to do so. This is similar to a premium for smokers, which have known increased medical expenses. It could be positioned as a discount to the vaccinated rather than a cost to the unvaccinated.
- As with other options, testing is required monthly for antibodies and weekly (or with a triggering event such as going out to a restaurant) for COVID at the unvaccinated person’s expense.
Compared to the $70 cost of a jab, which appears free to most as it is paid for by the government with our taxes, the vaccination is certainly less expensive. It is also a less risky approach to the individual and to society. Personally, I think Option 3 may be a bridge too far, and Option 1 and Option 2 are highly consistent with conservative values of individual freedoms and individual responsibilities, and could be implemented quickly.
Mandates or Market Solutions
The problem with the market solution is the classic moral hazard dilemma. Those unvaccinated simply may renege on their financial obligations should the risk they take to remain unvaccinated result in costly hospitalization. If one doesn’t appreciate the risk calculus I’ve found in my research is that approximately 1 in 400 who haven’t already had COVID, and are unvaccinated, will die in the next six months of COVID (versus 1 in 16,600 for a six months odds of dying in an auto accident), adding a price tag on-top of a risk they don’t fathom likely will make no difference in behaviors.
Still, if each test is paired with a PA or MD discussing risk each week, and the cost of testing mounts each week, it may be motivating to get vaccinated and have the testing expenses reimbursed promptly. Home testing and telemedicine make this approach possible in rural areas without easy access to commercial testing centers.
Consider the cost to society over the next six months if we don’t find a way to slow the cases, hospitalizations and deaths among the unvaccinated. We are heading toward 168,000 incremental deaths, almost entirely among unvaccinated, over the next six months. Hospitalizations will be roughly 5.3 times higher than the death toll at 890,000. That’s a hospital bill of $65 billion for the US. Add the statistical value of a life and we have a combined $1.5 trillion in expenses. For Nevada, the cost to this state is at least $15.3 billion over the next six months.
I suspect we will see misinformation that vaccine breakthroughs are just as common as unvaccinated people getting COVID. The Washoe data proves otherwise. An anti-vaxxer might point out that fully vaccinated people end up in the hospital and some die. That is true, but without context, that statement is almost meaningless. The rate of deaths per million per week among those vaccinated is close to zero. In Washoe it was zero. A bad year of the flu at this time of year kills 3 per million per week. Car fatalities kill 2 per million. Cancer and heart disease, the top killers, kill at 38 and 40, respectively, per million. Deaths among unvaccinated people are already over 20 per million and climbing daily. My forecast expects deaths among unvaccinated will exceed heart disease before the end of the month. COVID will once again be the No. 1 killer in the US among unvaccinated people. Last year, we didn’t have a vaccine to stop the carnage. This year we do.
Considering it would cost $9.6 billion to vaccinate every adult in the US who hasn’t been vaccinated yet, and save lives and hospital capacity, it is time for political leaders to take action. Leaders should discuss the merits of market approaches as an alternative to vaccination mandates. Home testing connected to a smartphone app is easy. A major tech company sent CUE home testing kits to every employee, and a friend let me borrow it to give it a try. It took less than seven minutes to unbox and set-up my account. Two minutes to do the test, and 20 minutes to wait for the results. I did it while making myself breakfast. It was easy. In my view, the results should be reported to the county health district along with commercial testing so we have a better idea of COVID test result trends. In many cases, home testing results create a blind spot for understanding infection trends and contract tracing. If we can implement home testing in a way that gives county health departments the data and visibility, and we can mix it with periodic commercial testing, we should do it. At the same time, we have lots of commercial testing capacity through pharmacies and testing centers.
Time is of the essence. Testing mandates, especially if paid for by the taxpayers rather than the individual, will likely be better received by the unvaccinated and will likely make a faster impact on ending the pandemic. Vaccination with Moderna and Pfizer takes about six weeks to achieve full effect, while more testing now, paired with encouragement of vaccination, can make a more immediate impact. Testing is required in many democratically elected partners in Europe. Why can't we, at minimum, get a testing mandate for the unvaccinated in place?
In addition, other market forces can help. There are many benefits to a fully vaccinated workforce, and businesses can (and many should) choose to require vaccination as a term of employment. Consumers can ask those they buy from to require vaccination. This can only help to reduce vaccine breakthroughs for the fully vaccinated. Brown’s effort to show which hospitals have a vaccine mandate for their staff is a great example of using market forces based on better information. Yelp, Google and others should surface which places of business have a fully vaccinated workforce as part of search results.
The clear evidence is that we are on a collision course with a Fourth Wave of COVID hospitalizations and deaths almost entirely fueled by the unvaccinated. I am not arguing that testing is better than vaccination. It’s not. I am offering an approach that gives people more choice in a situation that has already become needlessly politicized. To achieve full benefit of vaccination takes time while testing has immediate benefits.
This is the moment to take action. Look at the new case trend and do more than brace for impact. Put in place a system to get the unvaccinated tested, and consistently offered the option to be vaccinated. I suspect more will decide to be vaccinated under these conditions than if mandated by the government to get vaccinated.
It is not fair or just to place the economic burden for the Fourth Wave on those that are vaccinated. Nor is it wise to prolong a pandemic that would already be effectively over in the US, but for the unvaccinated. At the same time, we can respect individual choice by letting those unvaccinated learn about their level of immunity (if any) from prior infection through required antibody testing as an alternative to vaccination. We can educate them on the superior protection from prior infection plus vaccination. We can ensure those unvaccinated know if they become infected through required weekly testing. If they are infected, they can get early treatment, which is increases the odds of surviving COVID significantly. They can also inform others of exposure so they can get tested. Their testing and cooperation with health districts can aid contact tracing so that less people spread COVID to others. Through the process, we can engage those unvaccinated with regular medical experts that can help those unvaccinated get accurate information to make the right decision for them and their loved ones. Should they choose to get vaccinated, they should be able to do that right where they are doing their weekly tests.
In sum, we can take actions that will reduce the harms of the Fourth Wave of COVID, but inaction is inexcusable. If faced with the choice of no action (or obstructive action) from the right, and vaccine mandates from the left, I’d pick mandates in a second. I’d prefer a more nuanced solution with vaccines encouraged and testing required. How can we do nothing knowing this wave is almost entirely driven by the unvaccinated? Knowing the tangible and intangible costs and doing nothing to prevent them is unconscionable.
========
Rex Briggs lives in Reno and serves as Ad Council’s COVID-19 data science consultant and is an adviser to Brown University School of Public Health. The opinions expressed in this article are his own.